Stop Worrying About AI Replacing Doctors. Worry About How Many More We’ll Need.
There’s a dominant narrative taking hold in healthcare circles that AI is coming for clinical jobs. Surveys suggest a majority of physicians believe it will make them obsolete.
If this were to materialize anywhere, it would be radiology. The case seems airtight: the practice is already digitized, image interpretation is largely a pattern recognition task, and AI models have shown diagnostic accuracy at or near human expert levels. Today there are over 700 FDA-cleared AI devices in radiology.
Back in 2016, Geoffrey Hinton — the Nobel Prize-winning computer scientist and “godfather of AI” — made a definitive call: “People should stop training radiologists now.” It became one of the most-cited AI predictions in medicine.
What actually happened?
In 2025, U.S. diagnostic radiology residency programs offered a record 1,208 positions. Vacancy rates are at all-time highs. The Bureau of Labor Statistics projects radiology employment will grow 5-9% through 2034, faster than the average for all occupations. And the latest data from Marit Health shows the market is pricing in that scarcity with ballooning radiologist salaries.
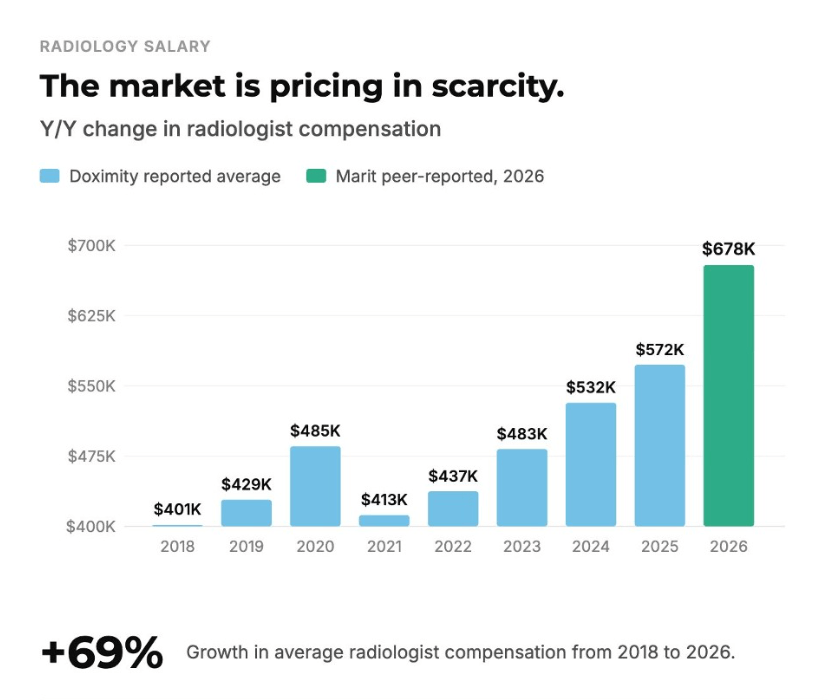
AI tools made each radiologist more productive. But demand for imaging — driven by an aging population, expanding chronic disease burden, and earlier detection — grew faster than AI could absorb. Rather than a surplus of radiologists, the field is experiencing a shortage. The technology that was supposed to eliminate the specialty instead exposed how badly undersupplied it already was.
The radiologists today aren’t doing fewer reads, but harder ones. The basic interpretations that AI handles well are being automated. What remains is subspecialty expertise, complex multi-system cases, procedural interventions, and the clinical integration work that requires talking to the care team and the patient. By automating the routine, AI elevated the profession.
This is not unique to radiology, or to healthcare. It is a pattern that has been repeated across industries every time a transformative technology makes workers dramatically more productive. Understanding why requires asking a different question than the one most people are asking. It’s not whether AI makes healthcare workers more productive or replaces workers. It’s whether those productivity gains get absorbed by existing demand, or whether they unlock demand that’s never existed before.
The pattern even has a name.
Jevons’ Paradox: When Efficiency Creates More Demand, Not Less
In 1865, British economist William Stanley Jevons noticed something counterintuitive. James Watt’s improvements to the steam engine made it dramatically more efficient — it used less coal to do the same amount of work. Common sense said consumption should fall.
It didn’t. It exploded.
Cheaper energy per unit of output didn’t just make existing uses more efficient. It made entirely new applications economically viable — new industries, factories, and machinery that previously couldn’t justify the fuel cost. It expanded the total market for coal far beyond anything the efficiency gain alone would have predicted.
This became Jevons’ Paradox: When a resource becomes cheaper to use, consumption tends to rise because the lower cost unlocks demand that didn’t previously exist.
We’ve seen this pattern across other technology waves. Fuel-efficient cars meant people drove more miles. Cloud computing made storage cheap and data skyrocketed. Streaming made video content cheap and frictionless and people watched more, not less.
Concerns about labor replacement haven’t always materialized the way people feared. When ATMs first rolled out across America in the 1970s, the number of bank tellers didn’t drop as many anticipated. Instead it grew — from 500,000 in 1980 to 600,000 in 2010. ATMs made branches cheaper to operate, but banks didn’t pocket the savings; they opened more branches to serve more people.
The job itself changed into something more valuable. Freed from routine cash transactions, tellers became relationship bankers, helping customers navigate complex needs, selling financial products, and building the personal connections that machines couldn’t replicate.
This pattern is already underway across healthcare, as we saw in radiology. AI won’t just expand the market for clinical services. It will push clinicians toward exactly the work they trained for: judgment, relationships, complexity. And it will bring healthcare to a population the current system has never been able to serve.
All the Healthcare Jobs That Don’t Exist Yet
Today, 83 million Americans lack access to primary care. New patients wait on average 26 days to see a doctor. The U.S. faces a projected shortage of up to 124,000 physicians by 2034. Too many people remain rationed out by cost and access barriers.
Transformative technologies have always created categories of work that didn’t previously exist. When the internet arrived, it spawned roles that had no prior analog: SEO specialist, social media manager, data scientist, cybersecurity analyst. These are now ubiquitous, well-compensated careers.
The same has happened in healthcare. Widespread EHR adoption in the last decade generated an entirely new layer of jobs — care coordinator, patient navigator, health coach, medical scribe, clinical documentation specialist — that barely existed a decade before. These roles emerged because complex care for more patients required new kinds of coordination.
AI is a far more powerful transformation than EHRs. But the mechanism is the same: as it absorbs the pattern-recognition overhead of medicine — reading scans, flagging anomalies, predicting risk — it lets clinicians focus on the work that can’t be automated. Clinical medicine is ultimately a judgment problem: a patient has a history, values, fears, and other social context that no algorithm fully captures. That human relational layer becomes more important, not less. The new roles emerging from this shift reflect exactly that dynamic: clinical AI trainer, digital health navigator, AI ethics officer, interoperability specialist, AI-assisted care coordinator.
And the barriers that AI dismantles will create demand for these jobs. A consumer-facing health tool can give someone who has never had a primary care relationship their first real window into their own health. A clinical AI assistant can help a nurse practitioner in a rural clinic manage a patient panel that previously would have required a specialist network. An AI-powered chronic disease platform keeps a diabetic patient engaged between quarterly check-ins, surfacing issues earlier and preventing hospitalizations. Rather than eliminating roles and services, these tools are creating new patient touchpoints that didn’t exist before.
The assumption underlying every “AI takes jobs” argument is that demand for healthcare is fixed. It isn’t. People want to be healthier and feel better. The barriers AI is dismantling are the ones that have kept millions from getting care they already want. When they come down, the system will expand. And it will require a very different kind of workforce infrastructure than what we have today.
We’ve Seen This Before — and Where We’re Investing
The healthcare system faces a challenge most people aren’t preparing for: how to train, organize, and deploy a much larger workforce to serve a much more demanding population.
At Reach, we invest at the intersection of learning, health, and work. Jevons’ Paradox in healthcare sits squarely in that intersection — and it exposes something that others may not see clearly: the healthcare workforce crisis isn’t primarily a healthcare problem. It’s a learning and human development problem that the system has never had to solve, because demand was historically managed through friction.
For decades, long wait times, high costs, and limited access functioned as an invisible rationing system. They suppressed demand and kept the system’s learning infrastructure deficit hidden. By removing these frictions, AI is exposing a system that doesn’t know how to train workers at speed, credential at scale, reach consumers who have never been served, or see its own workforce clearly enough to plan.
Those are problems Reach has spent a decade solving in education, through backing companies that help non-traditional learners navigate complex systems, redesign how adults acquire new skills in the flow of work, and build labor market intelligence for institutions operating in credential-dense environments. That expertise transfers directly to what healthcare needs at this moment.
We’re focused on the infrastructure layer that has to exist for the expanded market to function. Three areas are top of mind:
1. Consumer Activation and Navigation: Building the On-Ramp
If the Jevons’ mechanism works as we expect, tens of millions of Americans who have never had a real primary care relationship will be entering the system for the first time, activated by AI tools that gave them their first genuine window into their own health.
They’ve been outside the system long enough that it feels foreign. They may not know what a referral means, how to advocate for themselves in a clinical setting, or how to distinguish between a symptom that warrants urgent care versus one that can wait. Getting from “the AI flagged something” to “I’m in the right clinical setting with the right provider” is not a clinical problem — it’s a navigation and trust-building problem.
Reach has spent years investing in companies that help non-traditional learners navigate institutions built for people who already know how they work. We know that expanding access alone doesn’t produce better outcomes. A first-generation college student who gets admitted but has no one to help them register for classes, understand financial aid, or find the tutoring center is technically in the system, but practically on their own. The interventions that actually work are persistent, culturally competent, and meet people in the moments where they’re most likely to fall out.
Healthcare’s newly activated consumers face the same dynamic. The companies we’re most interested in aren’t just solving an access problem. They’re building health literacy and navigation infrastructure at population scale.
2. Scope-of-Practice Expansion Rails: Letting the Workforce Do More
Every healthcare worker operates within a legally defined scope of practice — the boundaries of what they’re permitted to diagnose, prescribe, and treat. These rules are slow to change, but economic pressure from demand expansion will force them to move faster. Already we’re seeing nurse practitioners practicing independently, pharmacists prescribing, and medical assistants conducting expanded intake. These expansions will only accelerate as physician shortages make the status quo untenable.
But scope expansion without infrastructure is dangerous. Even if nurse practitioners can legally practice independently, they still need real-time clinical decision support, supervision scaffolding, competency verification, and continuous feedback loops to do so safely and confidently. The companies that build those rails are the ones that make scope expansion viable at scale.
One opportunity we find compelling is helping existing physicians and advanced practice providers (APPs) add new specialties and capabilities in the flow of their current work. The traditional path to subspecialization is a fellowship that requires years of additional training, a major career interruption, and significant costs. That model made sense when specialization was rare and stable. It doesn’t work in a world where clinical needs are shifting rapidly and the workforce needs to be far more adaptive.
What would it look like for a primary care physician to develop genuine competency in lifestyle medicine, obesity care, or behavioral health integration — not through a two-year program, but through structured, AI-assisted learning embedded in their actual patient encounters? What would it look like for an APP in a rural clinic to expand into chronic disease management with real-time decision support that gradually transfers to independent judgment as competency builds?
These are competency-based education problems, ones that the Reach portfolio has been tackling for a decade. How do we design learning that transfers to real-world performance rather than just credentialing compliance? How do we build verification systems that employers and regulators trust?
Indeed Hiring Lab’s research is striking in how directly it maps onto what we believe: the defining labor market challenge ahead is not job creation or destruction — it’s reallocation. And the interventions that will matter most are upskilling, credential reform, and better worker-to-job matching.
3. Workforce Intelligence: Seeing the System Clearly
Health systems today are flying largely blind when it comes to their own workforce. They can tell you how many people they employ. They cannot identify where competency gaps are emerging, which roles will look different in three years, or how to model the care team composition they’ll need as their patient panel grows in complexity and volume.
This isn’t a data problem. Health systems are drowning in HR data, credentialing records, scheduling systems, and performance metrics. It’s an integration and intelligence puzzle. The information exists in silos that were never designed to talk to each other, and no one has built the layer that turns operational workforce data into strategic foresight.
As AI changes what clinicians do daily and care models move toward team-based delivery, this blind spot becomes genuinely expensive. Health systems that can’t anticipate their workforce needs will be unable to model the ROI of training programs and always be reacting — to shortages, to skill gaps, to care model shifts — while better-equipped systems plan around them.
Reach has watched the labor market intelligence infrastructure get built for education and the broader workforce — platforms that model how learners move from training into jobs, where credential supply and employer demand are misaligned, and how institutions can make smarter decisions about program investment. The firms that built that infrastructure for education were early picks-and-shovels play on a massive structural transition in how people acquire and verify skills. Healthcare is now entering the same transition, at a larger institutional scale and with higher stakes.
We’re looking for companies building workforce intelligence infrastructure for health systems — not just a staffing marketplace or scheduling tools, but the strategic layer that helps systems understand what their workforce needs to become, model the path to get there, and track progress against it in real time.
The Opportunity Worth Seizing
Yes, AI will make individual clinicians more productive. Yes, some tasks will be automated. These things are real.
But the assumption that demand stays flat while productivity improves has never held against transformative technology. It didn’t hold for coal, or for banking. It won’t hold for healthcare. The healthcare system is about to absorb tens of millions of people who have never had real access to it. The three areas above are core to the new workforce infrastructure that must exist for this expanded market to function.
If they sound like the pieces you’re building, we’d love to hear from you. Please reach out to jomayra@reachcapital.com.
Read the Latest
News and Insights