The Vitality Stack: Where We’re Investing to Power Health and Purpose

Healthcare has become obsessed with “longevity.” It refers to how long people live, with a focus on extending lives while maintaining a certain quality of health.
But it’s worth asking: to what end? Living longer is undoubtedly a worthwhile aspiration. But people don’t wake up every day optimizing for more years alone. They want years lived with health, agency, and purpose.
At Reach, we believe the real objective isn’t longevity. It’s vitality — the ability to participate fully in life physically, cognitively, socially, and emotionally over time. It is not simply the extension of lifespan, but the preservation of energy, agency, and resilience that make those years matter.
Innovations in healthcare have largely been successful in adding years to our lives. The next frontier is adding life to those years.
The Vitality Gap
We are living longer than ever, but not necessarily better. A study from McKinsey found that on average, people spend about half of their lives in less-than-good health, including 12% in poor health. This ratio has not changed much in the past 50 years.
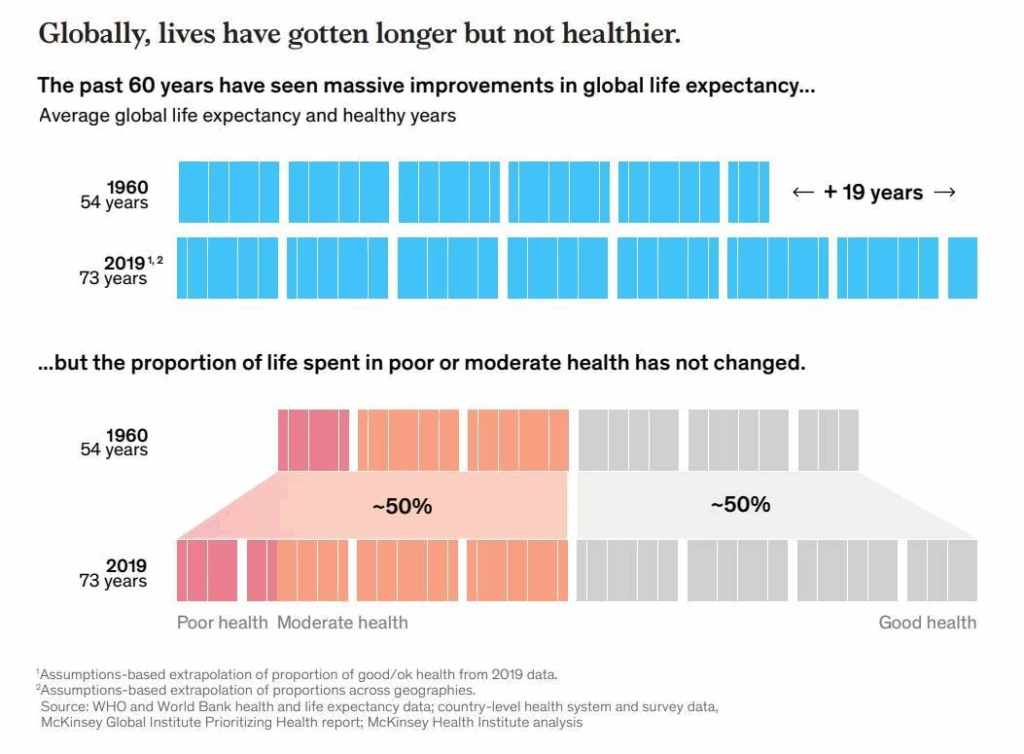
Over the last century, while lifespan has increased, healthspan — the years in which we live a healthy life — has also stagnated. The U.S. has the largest healthspan-lifespan gap, at 12.4 years, meaning we are living longer with chronic illnesses.
In other words, today’s system has become extraordinarily effective at extending life, but far less effective at preserving vitality within it.
People are tired of this tradeoff. Two-thirds of U.S. adults would choose a shorter, healthier life over a longer one lived with health problems.
This sentiment is further reflected in consumer spending behavior, where more than 60% prioritize purchasing products and services that support healthy aging, prevent chronic disease, preserve independence, and keep energy levels high. It’s no surprise, then, that the global longevity and preventive wellness market, already estimated at $5.8 trillion in 2024, is projected to reach $8.5 trillion by the end of this decade.
But the demand goes deeper than health alone.
People aren’t just seeking more years, or even healthier years. They are searching for meaning. A nationally representative survey found that 57% of Americans think about how to find greater purpose and meaning in life at least once a month, with many reflecting on this question weekly or even daily.
Aging Population, Shrinking Workforce: Vitality’s Inflection Point
Demographic, economic, clinical, and cultural forces are converging in ways that make our current healthcare system untenable.
The U.S. is aging rapidly. By 2030, one in five Americans will be over 65, and by 2040 that population will exceed 80 million. Meanwhile, people are spending more years outside the workforce than at any point in modern history, often without the institutions that once provided structure, identity, and community.
This demographic shift is colliding with mounting healthcare workforce shortages, where the U.S. faces a deficit of tens of thousands of primary care physicians and specialists over the next decade.
A system dependent on episodic, labor-intensive visits and one that ignores social connection will not scale. Although signs of progress are emerging, the current model remains rife with structural barriers.
Fragmented Care, Exhausted Providers
Even when services are available, logistical obstacles make them difficult to access and coordinate.
The average Medicare beneficiary sees nearly eight different clinicians each year, and 10% see more than 20. Nearly one in five adults delay or forgo care due to non-cost barriers such as scheduling, transportation, or time constraints. A lack of coordination between different providers often leads to duplicated testing, missed early warning signs, and poor handoffs across care settings. Health conditions are treated in silos instead of a continuous process.
For clinicians who trained to care for people, burdensome administrative tasks have come to dominate their work. Physicians now spend nearly twice as much time on documentation as they do with patients. More than 60% now report symptoms of burnout, and clinician turnover is estimated to cost the healthcare system upwards of $5 billion annually.
This crisis has accelerated experimentation with new care models like direct primary care, risk-bearing primary care, team-based and tech-enabled approaches that prioritize continuity, autonomy, and relationships. These models are better positioned to support prevention, coordination, and whole-person care, including attention to social and emotional wellbeing.
Misaligned Reimbursement
Most reimbursement is still tied to diagnosing and treating disease. Costs related to prevention, nutrition, social connection, or purpose-building remain under-reimbursed or not covered at all. Today, nearly 90% of healthcare spending is directed toward chronic and mental health conditions, yet the underlying drivers of these issues remain largely outside the economic model. This misalignment makes holistic, vitality-oriented care difficult to sustain.
There are signs that this is changing. Medicare spending on remote patient monitoring increased nearly 30-fold between 2019 and 2023, reflecting growing willingness to pay for continuous, between-visit care. Medicare Advantage now covers more than 50% of all Medicare beneficiaries, and these plans have flexibility to offer supplemental benefits related to nutrition, wellness, and social support. These shifts create economic pathways for models that integrate prevention, longitudinal care, and the social conditions that sustain vitality.
Social Infrastructure Erosion
Perhaps most critically, the systems that support health are poorly equipped to support connection and meaning, especially as people age.
Social infrastructure has eroded: families are smaller, geographic mobility is higher, and traditional community anchors, such as workplaces, religious institutions, and civic organizations now play a smaller role in daily life. Nearly one in three adults over 50 reports feeling socially isolated, and loneliness increases sharply with age, loss of mobility, and retirement.
Purpose also becomes harder to sustain over time. Many people derive identity and meaning from work or caregiving roles that fade later in life, yet few systems exist to help older adults transition into new forms of contribution, learning, or belonging.
In 2023, the U.S. Surgeon General declared loneliness a public health crisis, recognizing that social isolation is a risk factor associated with increased mortality, cognitive decline, and chronic disease. Longer lives without connection or meaning are increasingly recognized as a failure of the system, not the individual.
What Reach Is Excited About in the Vitality Stack
For years, healthcare technology promised transformation but often delivered complexity. But that is changing. Advances in sensors, AI, and data infrastructure now make it possible to collect continuous health signals, interpret them in real time, and integrate them into clinical workflows with less friction for both patients and providers.
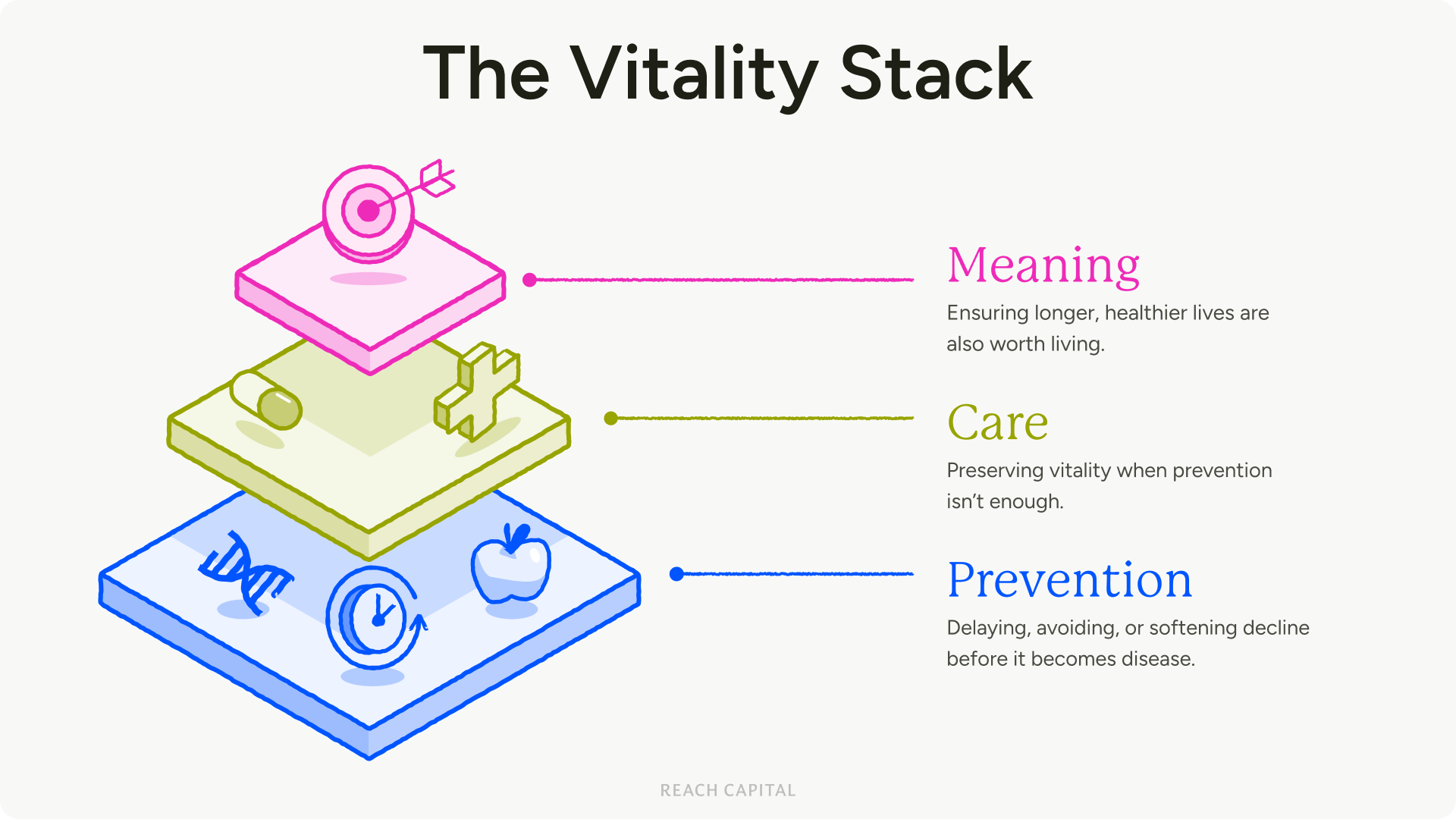
Vitality will be powered by connected systems — infrastructure, signals, and care models — working together across prevention, care, and meaning. If you are building anything in this stack, we want to hear from you! Here are a few areas we are especially excited about:
Prevention
Smarter Insights from New Diagnostics & Biomarkers
Vitality depends on detecting risk earlier. We are particularly excited about new classes of biomarkers that are continuous, low-friction, and embedded in everyday life activities. This includes non-invasive and ambient signals, such as voice, behavior, metabolism, and gut health that complement traditional labs and imaging.
Voice, in particular, represents a powerful new frontier: ubiquitous, passive, multisystemic, and capable of surfacing changes in cognitive, neurological, respiratory, and mental health earlier than conventional tools. We believe the future of prevention will be driven not by more tests, but by better signals captured naturally in daily life.
Food, Supplements, and Deprescribing
We see nutrition and supplementation not as consumer add-ons, but as foundational infrastructure for vitality. We are especially excited about companies advancing smarter supplements, personalized nutrition, food-as-medicine platforms, and tools that help reduce the need and risks of prescribing excessive medication.
As chronic disease rises and pill burden increases, the opportunity is not simply to add more intervention, but to replace, optimize, and simplify. This includes evidence-backed supplements, gut-health-driven approaches, and deprescribing workflows that improve outcomes while reducing cost and burden.
Care
The New Care Operating System
We’re excited about companies building the next operating system for care delivery: a platform designed around longitudinal relationships, prevention, and whole-person outcomes rather than episodic visits.
To be clear, we are not referring to electronic health records (EHRs), which are largely systems of record that document encounters, store clinical data, and support billing workflows. They were built for a healthcare system organized around visits and reimbursement.
The next generation of platforms will be systems of action. They will consist of tools that help clinicians and care teams translate data into decisions and coordinated interventions, powered by longitudinal patient records, AI-assisted care planning, remote monitoring inputs, and workflow support. These platforms integrate prevention, specialty care, behavioral context, and social determinants into a continuous, proactive care plan.
We expect many of these platforms will first emerge within cash-pay or membership-based care models, such as Direct Primary Care or concierge practices, which operate outside traditional insurance reimbursement. Because these clinics are not constrained by fee-for-service billing requirements, they have greater flexibility to experiment with longer visits, proactive care pathways, and preventative technologies.
These models are also growing rapidly as both clinicians and patients look for alternatives to traditional insurance-driven care. Over time, the data and care models developed in these environments could power new value-based reimbursement structures and ultimately reshape mainstream healthcare delivery.
Unified Health Identity & Longitudinal Data Infrastructure
Vitality cannot be managed without continuity. We are excited about companies building unified health identity layers that allow individuals to own and carry their health data across time, providers, and care settings. This includes identity, consent, interoperability, and longitudinal data platforms that make it possible to stitch together biomarkers, clinical records, behavioral data, and social context into a coherent, actionable health narrative. Without this foundation, prevention and personalization remain fragmented and fragile.
Meaning
Community and Purpose
Finally, we believe community and purpose are not “soft” outcomes. They are core inputs to vitality, especially as people age. We are interested in companies that help people maintain belonging, contribution, and identity across life transitions, including retirement, caregiving, and health decline.
This may take the form of technology-enabled communities for specific life stages or health conditions, platforms that match older adults with volunteering, mentoring, or part-time work opportunities, or care models that integrate social connection into primary or chronic care programs.
We are also interested in companies building tools that help families coordinate caregiving and maintain connection across generations, as well as programs that embed purpose and social engagement directly into aging services and senior living environments. As loneliness and loss of purpose emerge as public health crises, we believe this layer of the Vitality stack will become increasingly essential.
From Longevity to Vitality
People want longer, healthier, and more purposeful lives, and we want to back the companies that are helping to power that transformation. We believe vitality is not a single market, it’s an interconnected stack that requires better signals, better systems, better care models, and better support for how people live, connect, and find meaning over time.
If you’re building anywhere across this stack, we want to hear from you! Reach out to jomayra@reachcapital, caoimhe@reachcapital, and steve@reachcapital.com.
For more on how Reach invests in health, visit our health focus area or read the 2025 Healthcare Impact Report.
Read the Latest
News and Insights